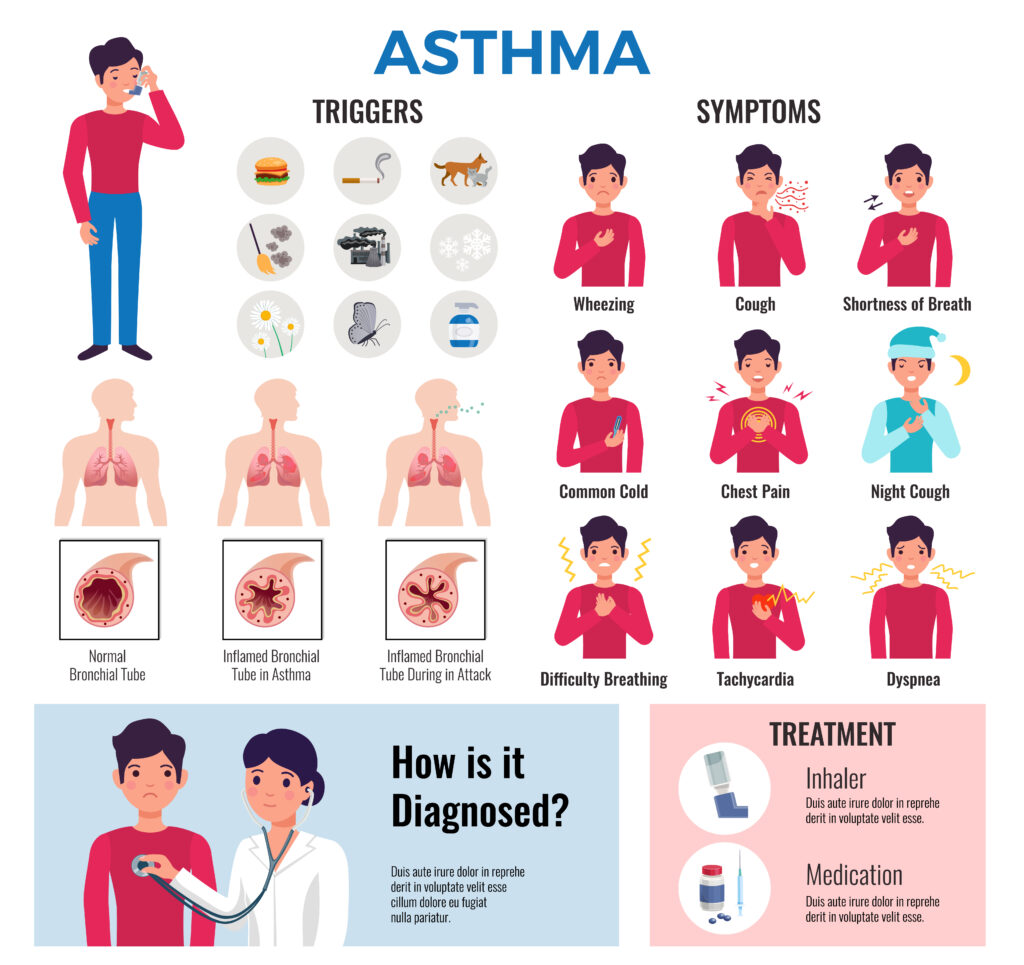
Ans. Asthma is a pathological condition where person suffer prolonged inflammation to the airways that commence to hyperresponsiveness of bronchi, increase mucus secretion, Bronchial constriction that further causes asthma episodes.
Que. Which are the risk factors that contribute to cause asthma?
Ans. 1. Allergy is one of the major cause to induce asthma. 2. Person exposed to some environmental irritant substances like-dust, pollen grains, grass etc. 3. Too much exercise also led to chocking sensation and commence to asthma. 4. Prolonged sadness, stress can also lead to develop asthma. 5. There are certain medications that may causes asthma.
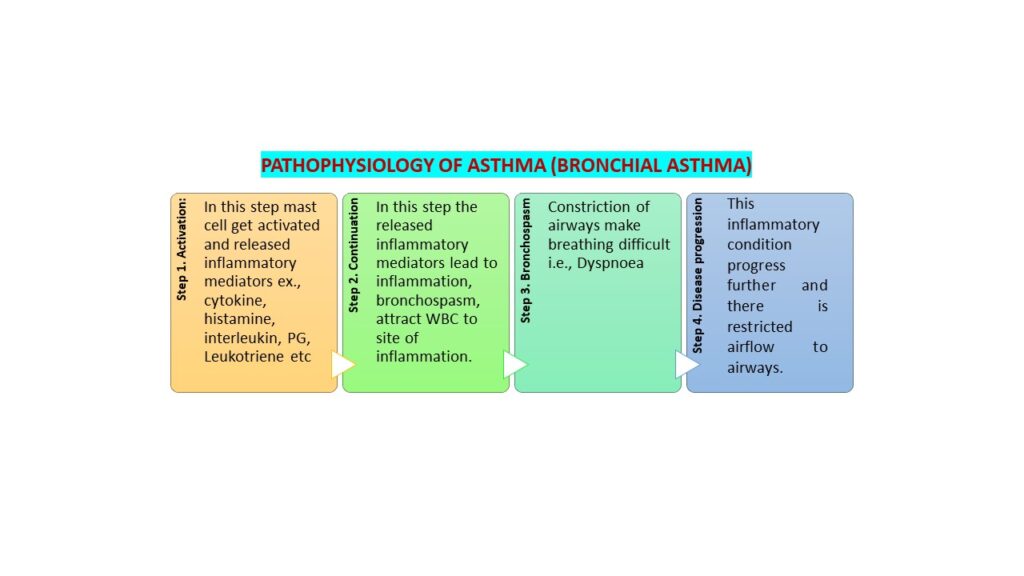
Que. How asthma occur? Give a brief pathophysiology of asthma. Ans.
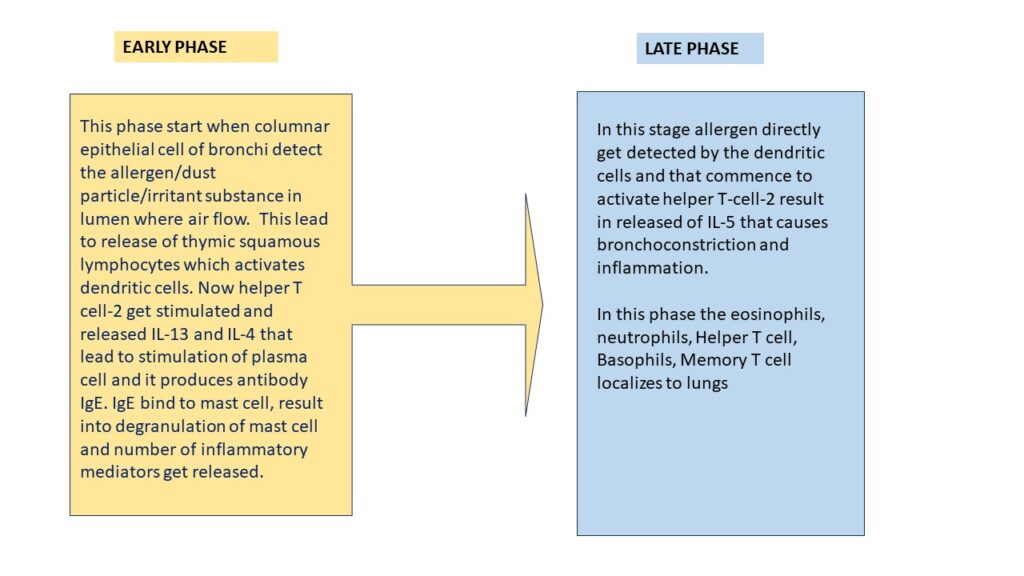
In broad concept we can divide asthma progression/exacerbation into 2 phase i.e., Early phase and late phase.
created by a ASSI. PROF. S.Chavan
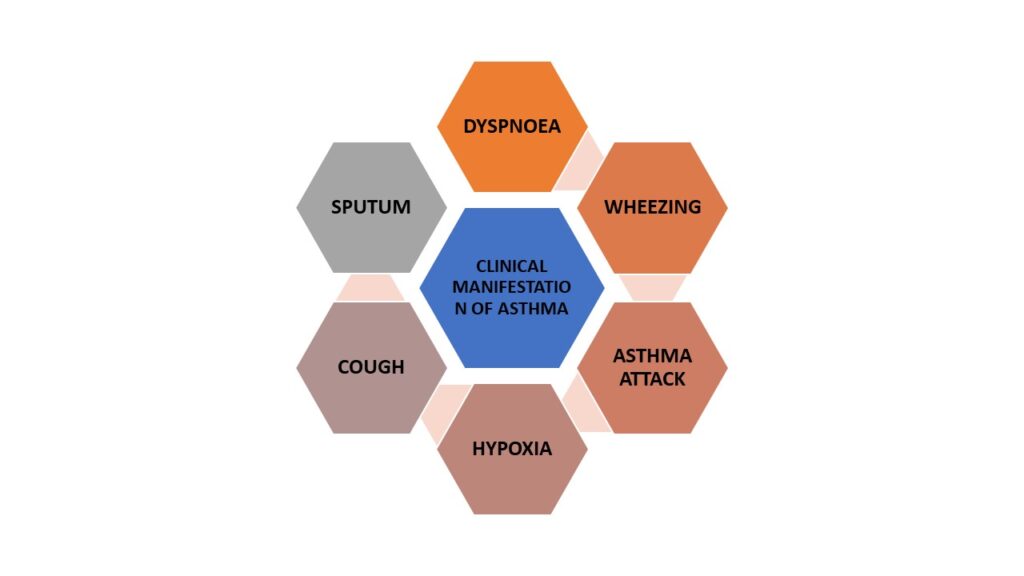
Clinical Manifestations:
created by a ASSI. PROF. S.Chavan
Que. How to assess asthma/ diagnostic findings of asthma: Ans. 1. First thing to look for family history of patient, whether he/she having any hereditary reason for causing disease, possible it may be acquired by any family member. 2. Environmental factors like seasonal change, allergic to dust or pollen grains, air pollution etc. 3. Comorbid conditions: Gastroesophageal reflux, certain medication can also induce asthma. 4. Expiratory airflow limitation 5. Spirometry: Force expiratory volume over 1 sec (FEV1) 6. Perform Allergy test 7. Bronchoprovocation test
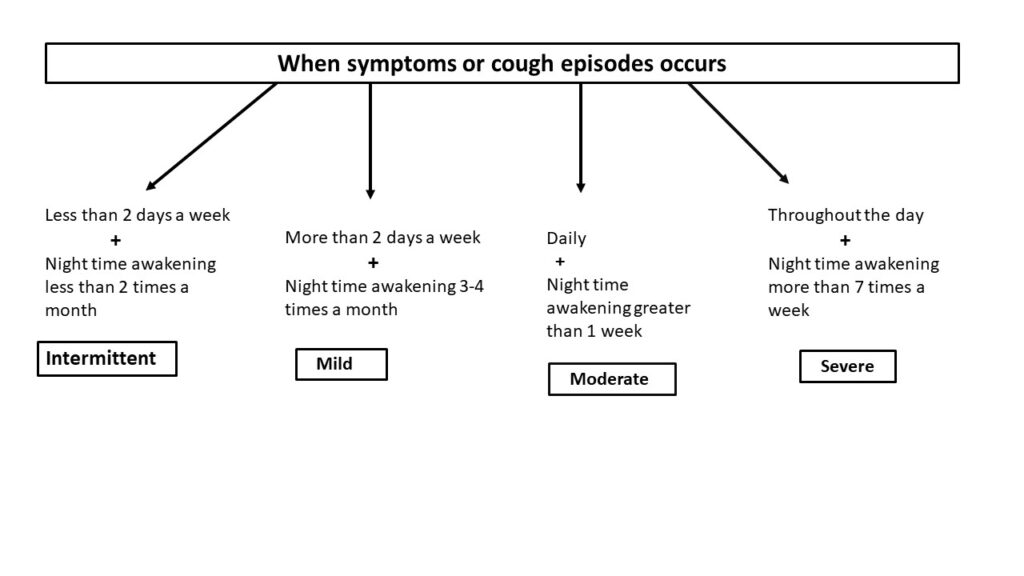
Que. Explain different stages of asthma that reflect severity of the disease:
created by a ASSI. PROF. S.Chavan
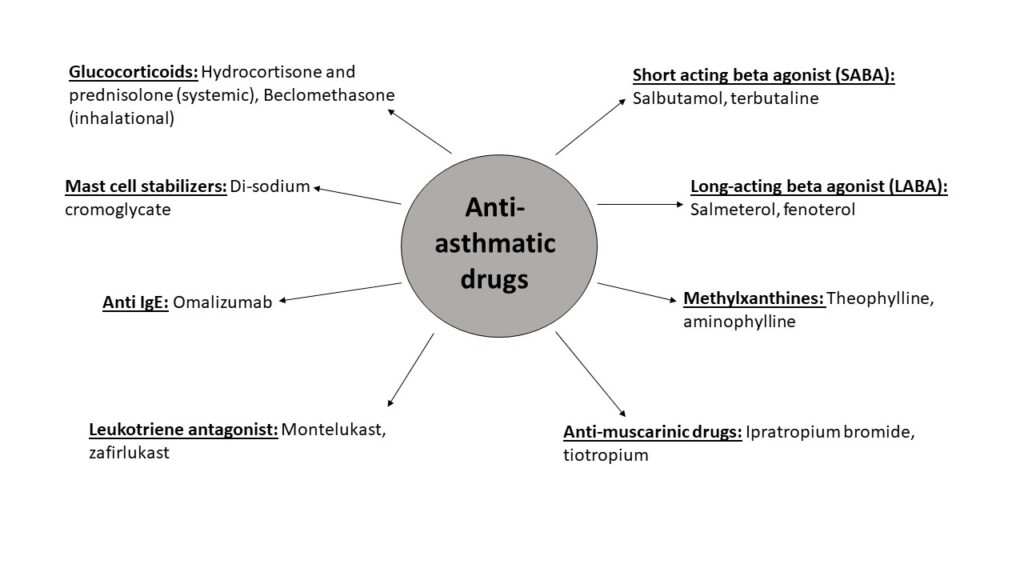
Que. Give classification of drugs used in treatment of asthma.
A. Short acting beta agonist (SABA): Salbutamol, terbutaline B. Long-acting beta agonist (LABA): Salmeterol, fenoterol C. Methylxanthines: Theophylline, aminophylline D. Anti-muscarinic drugs: Ipratropium bromide, tiotropium E. Glucocorticoids: Hydrocortisone and prednisolone (systemic), Beclomethasone (inhalational) F. Mast cell stabilizers: Di-sodium cromoglycate G. Leukotriene antagonist: Montelukast, zafirlukast H. Anti IgE: Omalizumab
created by a ASSI. PROF. S.Chavan
Que. Explain in short pharmacology of Salbutamol drug.
Ans. This drug comes under quick relief category it shows immediate bronchodilatory effect within minutes. It comes with portable inhaler container. Can be administer as nebulizer. On oral administration, salbutamol undergoes high first pass metabolism in the gut with about 50% bioavailability. The duration of action is longer than by inhalation route 4–6 hr MOA: salbutamol act on beta-2 receptor which is GPCR receptor. Activate adenyl cyclase. This convert ATP into cAMP, when level of cAMP increases within smooth muscle it causes inactivation of MLCK and hence it cannot contract further result into relaxation i.e., bronchodilation of bronchial smooth muscle.
ADME: It administred through inhalational route, this followed by absorption of drug by smooth
muscle of bronchi. Volume of distribution upon I.V administration as 156+/38 L 1 . It is weakly bound
to protein. Metabolized in lungs. But it converted non pharmacologic drug in liver. Excreted in urine through urine Adverse effect: Palpitation, skeletal muscle tremor, nervousness Uses: Bronchial asthma, Bronchoconstriction, COPD